
Crohn’s Disease
Crohn’s Disease
Theodoros Argyropoulos, M.D., M.Sc., Ph.D.
Consultant Gastroenterologist, General Hospital “G. Gennimatas”
Scientific Director, Affidea Peristeri Gastroenterology Unit
Contents
What is Crohn’s Disease?
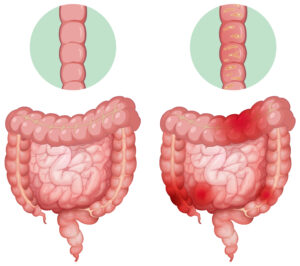
Crohn’s disease is a chronic, relapsing inflammatory condition of the digestive tract. It can affect any part from the mouth to the anus, most commonly the terminal ileum and/or the colon, and the inflammation is transmural (penetrates all layers of the intestinal wall). It is characterized by periods of flare-ups and remission. Although it cannot be permanently cured, with modern monitoring and targeted treatment, long-term remission and a normal quality of life can be achieved.


What symptoms does it cause?
- • Diarrhea (often without blood)
- • Abdominal pain/cramps, often in the lower right quadrant
- • Weight loss, reduced appetite, fatigue
- • Fever during flare-ups
- • Perianal symptoms: fissures, abscesses, fistulas
- • Mouth ulcers
- • Blood in the stool (less common than in ulcerative colitis)
Crohn's Disease
Causes & Risk Factors
Crohn’s disease arises from an immune system dysfunction in genetically predisposed individuals, triggered by microbial and environmental factors.
Risk Factors:
Age: Most common under 30 (but also >50–60)
Smoking: A strong aggravating factor for Crohn’s
Use of NSAIDs: Such as ibuprofen
Western lifestyle & northern climates
Genetic predisposition / family history
Microbiome disturbances, stress (worsening factors, not direct causes)

When to Consult a Gastroenterologist (Red Flags)
- Persistent diarrhea lasting more than 2–3 weeks
- Unexplained weight loss, loss of appetite, fatigue
- Blood in stool or mucus-filled bowel movements
- Fever, waking at night to defecate
- Perianal pain/discharge, possible abscess or fistula
- Signs of dehydration or severe abdominal pain
How Is Crohn’s Disease Diagnosed?
The diagnosis of Crohn’s disease is based on a combination of findings from clinical presentation, endoscopy, histological analysis, imaging studies, and laboratory markers.
-
Fundamental tests:
- • Colonoscopy with biopsy: allows direct evaluation of the colon and terminal ileum, revealing characteristic findings of asymmetrical, transmural inflammation.
- • Stool markers (calprotectin, lactoferrin): reflect the degree of intestinal inflammation and aid in the differential diagnosis from functional disorders.
- • Blood tests: CRP and ESR (inflammatory markers), hematocrit, ferritin, vitamins B12 and D, folic acid, and albumin to assess nutritional status and inflammatory activity.
- • Small bowel imaging (MR enterography or CT enterography): used to detect strictures, abscesses, or fistulas that may not be visible endoscopically.
- • Intestinal ultrasound: a non-invasive method particularly useful in specialized centers for assessing disease activity and extent.
- • Differential diagnosis: other causes of intestinal inflammation must be excluded, such as infectious, ischemic, or drug-induced colitis, as well as ulcerative colitis.




Treatment: Goals & Options (Treat-to-Target)
The modern approach to managing Crohn’s disease is based on the treat-to-target strategy — treating with clearly defined goals and systematically assessing the patient’s response.

Therapeutic Goals
- Successful disease management goes beyond mere symptom relief and aims for multi-level remission:
- • Clinical remission: absence of symptoms (pain, diarrhea, weight loss).
- • Biochemical remission: normal levels of CRP and fecal calprotectin.
- • Endoscopic/Imaging remission: mucosal healing, absence of ulcers or active inflammatory lesions.
- Achieving all of the above significantly reduces the risk of relapse, complications, and the need for surgery.

Medication Classes (Personalized)
- The choice of treatment depends on:
- • the severity and location of the disease,
- • the history of previous treatments,
- • the overall health and preferences of the patient.
The main therapeutic categories include:
1. Corticosteroids (e.g. prednisolone, budesonide)
➜ Used for induction of remission in active disease, not for long-term maintenance due to side effects.
2. Immunomodulators (azathioprine, 6-mercaptopurine, methotrexate)
3. Biologic Agents
Anti-TNF: Infliximab, Adalimumab
Anti-Integrin: Vedolizumab (gut-selective agent, with lower systemic risk)
Anti-IL-12/23: Ustekinumab
Anti-IL-23: Risankizumab
➜ Targeted therapies that modulate the inflammatory response, achieving high rates of remission and mucosal healing.
4. Targeted Small Molecule Therapies
5. Antibiotics
6. Surgical Management
➜ When there is stricturing or fistulizing disease, uncontrolled abscesses, or treatment-resistant inflammation.
Goal: bowel-sparing approaches and preservation of quality of life.
Perianal Disease
This is a particularly challenging form of Crohn’s disease that requires a multidisciplinary approach:
- Endoscopic and imaging-based staging
- Abscess drainage
- Seton placement (when indicated)
- Systemic biologic therapy (usually anti-TNF)
Treatment of Crohn’s disease is continuously evolving, with the goal of achieving deep remission at all levels through personalized therapy and close monitoring to allow timely adjustments.

Complications
-
Intestinal Complications:
- Strictures / Obstruction: Resulting from chronic inflammation and scarring, which may lead to abdominal pain, bloating, and vomiting.
- Fistulas: Abnormal connections between the intestine and other organs or the skin (entero-enteric, entero-cutaneous, perianal). Often associated with abscess formation.
- Malnutrition / Malabsorption: Due to reduced nutrient absorption. Common deficiencies include iron, vitamin B12, and folic acid.
- Perforation / Rupture: A rare but serious complication requiring urgent medical intervention.
-
Extraintestinal Manifestations:
Crohn’s disease is a systemic inflammatory disorder, meaning it can affect other organs beyond the digestive tract:
- Arthritis (peripheral or axial)
- Skin lesions such as erythema nodosum and pyoderma gangrenosum
- Uveitis (inflammation of the eyes)
- Hepatobiliary diseases — gallstones, primary sclerosing cholangitis
- Nephrolithiasis (oxalate kidney stones)
- Thromboembolic disease (increased risk of blood clots)
- Osteopenia / Osteoporosis, often due to corticosteroid use or malabsorption.

Nutrition & Lifestyle
Proper nutrition and healthy habits play a key role in stabilizing Crohn’s disease and improving quality of life.
Avoid smoking
Do not use Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Follow a balanced, anti-inflammatory diet
During flare-ups or in stricturing disease: adapt to a low-residue or easily digestible diet as advised by your doctor
Nutritional supplements may be needed (e.g., iron, vitamin B12, folic acid)
Exercise & mental well-being are essential for overall disease management and emotional health
Vaccinations & Treatment Safety
Before or during immunomodulatory or biologic therapy, the following vaccinations are recommended:
Influenza (annual)
Pneumococcus
Hepatitis B (HBV)
Hepatitis A (HAV), where indicated
HPV
Tetanus
Screening for tuberculosis, HBV, and HCV is required before starting biologic agents.
Live vaccines (e.g., MMR, varicella) should be avoided during active immunosuppression — always consult your physician beforehand.
Bone density testing (DEXA) is recommended for patients on prolonged corticosteroid use or with other risk factors for osteoporosis.
Follow-Up After Diagnosis
Ongoing follow-up is just as important as diagnosis and treatment in managing Crohn’s disease effectively.
Colonoscopy: Performed 6–12 months after diagnosis, then every 1–3 years depending on findings.
Cancer surveillance: Begins 8–10 years after diagnosis, with biopsies and chromoendoscopy every 1–2 years to screen for dysplasia.
CRP & Calprotectin: Every 3–6 months to monitor intestinal inflammation.
Blood tests: Include hematocrit, ferritin, vitamin B12, vitamin D, and albumin levels.
Liver and kidney function: Regular monitoring during treatment with immunomodulators or biologics.
Imaging (MR Enterography / Ultrasound): To assess strictures, fistulas, or signs of active inflammation.
Goal: Achieve and maintain clinical, biological, and mucosal remission through a treat-to-target strategy.
Frequently Asked Questions (FAQ)
Will I need to take medication forever?
Crohn’s disease is chronic. Maintenance therapy significantly reduces flare-ups, hospitalizations, and complications.
The duration of treatment is individualized, depending on the severity, location, and the patient’s response.
What can I do to feel better?
Follow an anti-inflammatory diet and avoid foods that worsen your symptoms.
Quit smoking.
Manage stress through exercise, quality sleep, and psychological support.
Maintain regular communication with your gastroenterologist.
Does Crohn’s disease increase cancer risk?
Does the risk of genital warts increase?
Is Crohn’s disease related to irritable bowel syndrome (IBS)?
Yes, they often coexist.
More than two-thirds of patients with inflammatory bowel disease experience IBS-like symptoms.
This does not worsen the inflammation, but it can affect quality of life, mood, and daily functioning.
Is Crohn’s disease related to celiac disease?
Yes, there is an association.
Patients with Crohn’s disease have a threefold higher risk of developing celiac disease compared to the general population.
If malabsorption or unexplained anemia is present, celiac screening is recommended.
What will my life be like with Crohn’s disease?
Most patients live a normal, active life.
With proper treatment, regular monitoring, and support, flare-ups are reduced and quality of life remains high.
Can I get pregnant?
In most cases, yes.
Crohn’s disease does not reduce fertility when the disease is in remission.
Before trying to conceive, consult your doctor to plan the pregnancy and adjust medication if necessary.
I’m on treatment and developed an infection — should I stop my medication?
Not without medical guidance.
Management depends on:
The type of infection (viral, bacterial, fungal, Clostridium difficile)
The type of therapy (thiopurines, anti-TNF agents, anti-integrins, etc.)
Your treating physician will decide whether treatment should be temporarily paused or adjusted based on your condition.
Book an Appointment
For a diagnosis, personalized treatment, and safe follow-up using the latest techniques (small bowel imaging, high-definition endoscopy, and more):
Argyropoulos Theodoros, M.D., M.Sc., Ph.D.
Gastroenterologist
Schedule your appointment and let’s create a strategic plan tailored to your individual needs.